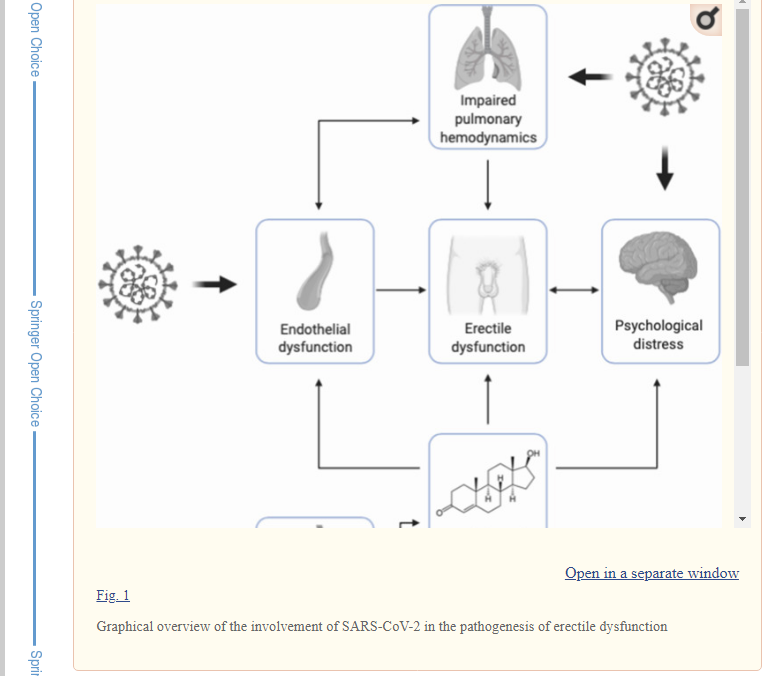
Claim: Some COVID-19-recovered male patients experience erectile dysfunction as a complication.
Mostly true. The Ghana Medical Association states erectile dysfunction as complaints from a lot of recovered COVID-19 male patients. This is also corroborated by research and reports from other parts of the world that attempt to prove this claim to be so. However, neither the WHO nor CDC has established the symptom to be a COVID-19 complication as yet. The Ghana Health Service is also yet to confirm and establish the correlation through extensive research.
In the Starr FM and JoyOnline news reports that have set the agenda for the conversation, the information was disclosed by the Ghana Medical Association (GMA). It is noteworthy that in the news reports, the Vice President of the GMA, Dr. Frank Serebour, stated that there are nation-wide complaints from a lot of recovered patients about experiencing post-recovery erectile dysfunction requiring attention and treatment.
The news reports added that further enquiries from the Ashanti Regional Director of the Ghana Health Service, Dr. Emmanuel Tenkorang, also shows that the correlation between erectile dysfunction and COVID-19 pertaining to Ghana is yet to be confirmed and established through research and empirical data.
Notwithstanding, research and reports from across the world show that medical professionals are facing similar observations of erectile dysfunction as a possible COVID-19 complication.
For example, in a NBC LX news report in Chicago, United States, which was also similarly reported by DW in Germany, an infectious disease expert, Dr. Dena Grayson, cautioned on how a mild case of the virus has potential of causing long-term complications including erectile dysfunction. She explained that this is because the virus affects tissues in the vasculature.
Similarly, the reports showed that the link between COVID-19 and the male reproductive system may be caused by the damage to the vascular and respiratory systems of COVID-19 patients.
Furthermore, a study, ‘Addressing male sexual and reproductive health in the wake of COVID-19 outbreak’, published in 2020 in the Journal of Endocrinological Investigation, found evidence of the potential of the onset of Erectile Dysfunction as a COVID-19 complication by reviewing several similar studies conducted on male COVID-19 recovered patients in the United States, Asia, and Europe.
The study explained this as follows:
“It is well established that ACE2 is the entry point for the SARS-CoV-2 in host cells. In males, adult Leydig cells express this enzyme, therefore, suggesting that testicular damage can occur following infection . Testicular damage in COVID-19 might, therefore, induce a state of hypogonadism as proven by decreased testosterone-to-LH ratio in patients with COVID-19, suggestive of impaired steroidogenesis resulting from subclinical testicular dysfunction. Post-mortem examinations of testicular tissue from 12 COVID-19 patients showed significantly reduced Leydig cells, as well as edema and inflammation in the interstitium. A recent report on 31 male COVID-19 patients in Italy identified that some patients developed hypergonadotropic hypogonadism following the onset of the disease. In the same study, lower levels of serum testosterone (total and free) acted as predictors of poor prognosis in SARS-CoV-2 men. Whether this state of hypogonadism is permanent or temporary is a question so far left unanswered. Testosterone acts as a modulator for endothelial function and suppresses inflammation by increasing levels of anti-inflammatory cytokines (such as IL-10) and reducing levels of pro-inflammatory cytokines such as TNF-α, IL-6 and IL-1β. It can, therefore, be hypothesized that suppression of testosterone levels might be one of the reasons for the large difference in terms of mortality and hospitalization rate between males and females and might also explain why SARS-CoV-2 most commonly infects old men”
Consequently, the study recommended the need for assessment and treatment to be followed up on this finding.
However, we find that neither the World Health Organisation nor the Centre for Disease Control has listed erectile dysfunction (or general effects on sexual reproductive system) as a confirmed COVID-19 complication as yet, in spite of evidence from available research from medical experts across the world and complaints from many affected recovered male patients about erectile dysfunction.
Conclusion
The claims by the Ghana Medical Association that recovered COVID-19 patients are experiencing erectile dysfunction are not unfounded. This is derived from the complaints of a lot of recovered patients across the country. Furthermore, news reports and research across the world also give evidence to link between erectile dysfunction and COVID-19 infections in males. However, the Ghana Health Service is yet to confirm and establish erectile dysfunction as a COVID-19 complication, just as the WHO or CDC has not listed erectile dysfunction as a COVID-19 complication yet. It is premature to declare this claim false or true, until there is an update from the WHO on links between Covid-19 infected males and erectile dysfunction.
The concerted efforts by scientists and medical experts across the world in rolling out vaccines for COVID-19 has been met with skeptical attacks. Conspiracy theories, misinformation and public apprehensions are among the skepticism restraining undiscerning audiences from getting vaccinated, given the adverse consequences purported to be associated with COVID-19 vaccines. And yet again, fact-checkers are having to war against the verbal missiles threatening the possible end of the pandemic – vaccine infomedic – that have plagued both social and traditional media spaces across the world. The vaccine misinformation has circulated in varied forms and upon access to them Dubawa has verified them accordingly.
At the onset of the pandemic, there seemed to be widespread and welcoming news of the discovery of purported vaccines, which however all turned out to be false. The alleged discovery of vaccines was found to be so welcoming that political figures were associated with the claims, perhaps to give the claims more weight. This was evidenced in a claim made against former American president, Donald Trump, alleged to have announced a new vaccine, which was found to be false.
It was not until the actual recent discovery of vaccines by some pharmaceutical companies that the false narrative of side effects and medium of administering the vaccines started being pushed strongly across media spaces, all of which were again, found to be false. Oblivious to what the obsession and association with penis-related COVID-19 discussion was, Dubawa found penis enlargement and injection of the vaccine through the penis to be the false side effects and medium of administering the vaccine, respectively, being circulated.
While concerns and apprehensions about COVID-19 vaccines are valid and well expected for a new virus, it is no justification to incite public unrest by misinforming others with one’s perceived knowledge and uncertainties. When unsure, one is expected to simply verify from authorised sources before sharing.
Claim: A viral video clip claims vaccines are targeted at eliminating Africans.
The claim that vaccines are meant to eliminate Africans is false and the statement on vaccines is not related to COVID-19 vaccines.
Full Text
With the growing spread of misinformation and different theories surrounding the coronavirus (COVID-19) vaccine in relation to Africa, a 30-second video going viral on social media claims there is a plan to eliminate Africans through vaccines.
In the video, a witness named Dr Robert O. Young who was answering questions from a set of panellists said there were too many people in the world and there was the need to get rid of them starting off in Africa.
“For the purpose of sterilization and population control, there is too many people on the planet we need to get rid off in the words of Bill Gate, at least 3billion people need to die. So we will just start off in Africa. We will start doing our research there and we will eliminate most of the Africans because they are deplorable, they are worthless, they are not part of this world economy so they have their rights taken away and they are surpressed and experimented”
Excerpt of Dr Robert’s statement.
Screenshot of the viral video.
Verification
Dubawa researched the witness (Dr Robert O. Young) in the video and discovered that Dr Young is an American naturopathic practitioner and author of alternative medicine books.
Dubawa also conducted a Google reverse image search with screenshots of the video which led to a report on January 13, 2021, by Everyday.ng.
Screenshot of Everyday’s report.
According to this report, the video was filmed at the International Tribunal of Natural Justice (ITNJ) sittings in Bali, Indonesia at the Judicial Commission of Inquiry into the Weaponization of the Biosphere in June 2019.
The video has, however, been gaining traction since emergence of the COVID-19 pandemic and vaccination.
This report led us to the ITNJ website where we saw different clips of this sitting from different days without finding Dr Young’s statement.
Screenshot of ITNJ’s website.
The 10-minute clip of Day one covered the opening introduction of the Bali sitting in June 2019.
Screenshot of Day 1 sitting on ITNJ’s website.
Day two clip covered ITNJ Trustee Emeritus, Sacha Stone, giving a speech.
Screenshot of Day 2 sitting on ITNJ’s website.
The link available on the site for the full clip of the seating led to a YouTube video that could not be accessed.
Screenshot of Youtube page with the private video.
Dubawa then went ahead to search for Dr Young’s testimony at the ball seating. Dubawa found a Youtube video of one hour and 38 minutes that contained Dr. Robert O Young’s testimony.
Screenshot of the Youtube video containing Dr Young’s testimony.
The video was posted on Youtube with a short summary that explained that Dr Young’s statement provides the how and why the state department put him out of business and in jail because of his natural treatment to cure cancer.
Going through the video, Dubawa learnt Dr Young was trying to make the point that the different vaccines given to children in the first six years of their life, from the measles vaccine to the polio vaccine are more poisonous than helpful.
The short clip going viral was trimmed out of the full testimony towards the end of the video, where Dr Young quoting Bill Gate, said these vaccines are meant to kill and reduce the world population. It is, however, noteworthy to note that the claim on depopulation by Dr Young accredited to Bill Gate has been debunked.
While the statement in the viral clip is true and taken from the original full video of Dr Young’s testimony, it is not related to COVID-19 vaccines.
Conclusion
Dubawa’s findings show that while it is true that Dr Young made such a statement in an original video from the ITNJ seating, his statement was taken out of context as his statement and the seating have no relation with COVID-19. The time of this seating also discredits this video’s connection to COVID-19 which happened 5 months before COVID-19 broke out in December 2019. This makes the claim false and misleading.
CLAIM: A photo circulating and rumours making rounds suggest the COVID-19 vaccine leads to penis pnlargement.
FALSE. Whilst there have been notable side-effects associated with the dose of the COVID-19 Vaccine, none of those side-effects has proven or led to any case of penis enlargement as claimed in the photo that is circulating on social media.
Full Text
The photo purporting to be breaking news from a news agency reads, “COVID-19 Vaccine enlarges Penis.” This has drawn attention from mostly young men, and the author of this article was privy to one of the discussions and had access to the photo following the conversation he heard amongst young men at a public event. The discussion attracted the attention of many and most of them confirmed to have seen the photo circulating on social media especially WhatsApp.
This photo with the flamboyant claim is just one of the many backlashes to have emerged from the announcement of a clinically trusted COVID-19 vaccine in a much shorter time than anticipated. The Pfizer Covid Vaccine has already been applied to the most vulnerable group of people to the pandemic – frontline health workers in the United Kingdom and the United States.
Verification
The Pfizer BioNTech vaccine has gone through the required clinical trial that was presented to over 44,000 participants and scored over 95% in effectiveness and safety. This did not, however, clear the vaccine of potential side effects, particularly that the first dosage on British health workers did come with reactionary side-effects. The side effects triggered by histories of allergic reactions were reported in this New York Times article. But of all the side reactions to the vaccine so far, nothing like penis enlargement has been reported.
The Pfizer BioNTech Vaccine, like any other vaccine, is delivered as a shot in the arm and notable side effects have been headaches, fatigue, chills and muscle pain. The penis enlargement claim, from all indications, has proven to be baseless for lack of medical or scientific backing.
For further clarifications, Dubawa checked the other COVID-19 Vaccine, Moderna vaccine, which has very recently received emergency approval. Its clinical test has shown its effectiveness to be almost as high as that of the Pfizer vaccine. It was first delivered to top health officials like Dr Fauci on the 22 December 2020 and so far, no such claim has been associated with it.
Patrick Semansky / AFP – Getty Images
Secondly, the photo circulating has no inscription or logo of any particular brand that raises red flags. It further claimed a 23% increase in penis size relating it to a study which was never explained in detail as to who or what organization conducted the study and how they reached such a conclusion on a vaccine that is less than a month old. These misconceptions and red-flags question the veracity of such claims and expose its groundlessness.
Conclusion
The claim of penis enlargement related to the COVID-19 vaccine is unfounded and therefore misleading. No major side effect has been identified, apart from cases of patients with histories of allergic reactions and none of such effects is related to penis enlargement.
While Akufo-Addo only stated that the former president’s passing was due to a short illness, other reports are suggesting that the former president died from COVID-19. It is on this basis that information surfacing the media space state freely that the former president was seen at his mother’s funeral without observing COVID-19 protocols.
One of such claims accompanied by a video of Rawlings dancing has circulated on WhatsApp.
The Whatsapp message reads:
‘’Check out the above. Rawlings is seen above during his mother’s funeral with no mask and no social distancing. A week later was admitted for Covid-19 and now Requiem for him. Please don’t joke; observe all Covid 19 protocols. Stay alive!’’
Verification:
In the 35-second video that is associated with the claim, it is observed that Rawlings was wearing a black and white Achimota School print shirt together with his wife, Nana Konadu Agyemang Rawlings, and not a funeral cloth as expected.
Further checks show that the video was reported four years ago before the COVID-19 pandemic. In the news report dated 8 March 2016, it proves to be a video of Rawlings dancing Agbadza at Achimota School’s 1966/67 year group’s 50th anniversary celebration.
The claim that Rawlings was seen in a video during his mother’s funeral with no mask and no social distancing is false. The video associated with the claim is an old video from 2016 before the COVID-19 pandemic, where the late former president and his wife attended a 1966/67 Achimota School year group 50th anniversary event. The video has no link with Rawlings’ mother’s funeral which happened last month.
Ahead of the 2020 elections in December, the National Democratic Congress (NDC) launched their manifesto, the ‘People’s Manifesto’ on Monday, 7 September 2020.
At the launch, the presidential candidate of the party, John Dramani Mahama, in his introductory speech (1:59:22- 2:06:45 of the recorded Facebook live video) was heard making a number of claims centred mainly on the economic state of Ghana and on a government’s COVID-19 management.
A transcript of Mahama’s speech which captures the context in which the identified claims were made reads:
“…In many cases, countries considered relatively less advanced with smaller economies are emerging more resilient and less affected by the global shocks than some countries that are considered advanced. The case of Vietnam, a relatively smaller country bordering China, and therefore closer to the original source of the Coronavirus pandemic has survived much better with relatively less infections and deaths than known global superpowers...Excessive borrowing over the last four years has placed Ghana in a high debt risk category, with absolutely nothing to show for it…”
Consequently, Dubawa accessed the available facts concerning some identified claims, in producing its attendant verdicts.
Claim 1:Vietnam has survived the Coronavirus pandemic much better with relatively lesser infections and deaths than known global superpowers
Verdict: Reports from the WHO, CDC, COVID-19 data sites andmedia show that Vietnam has recorded relatively lesser infections and deaths compared to the known global superpowers.
The countries largely referred to as the global superpowers are the five permanent members of the UN Security Council namely the United States of America (US), the United Kingdom (UK), Russian Federation, China and France.
Dubawa accessed the statistics for the population, confirmed cases/infections and deaths as at 7 September 2020, recorded for Vietnam, US, UK, Russian Federation, China and France tabulated below:
Source: Population: Worldometer Confirmed case & deaths: WHO
Comparatively, from the tabulated statistics, Vietnam, which has a population higher than the UK and France, has recorded smaller rates of infection and death than the two countries.
Moreso, the Vietnam Coronavirus tracker also reveals that out of the 1,059 confirmed cases, there have been 902 Covid-19 recoveries in Vietnam, with no critical cases treated in Intensive Care Unit and an 84% recovery rate of the total cases.
In June 2020, the Centre for Disease Control (CDC) described Vietnam’s response to controlling the pandemic as an excellent credit to the country’s leadership strategies.
“Vietnam has excelled in controlling COVID-19 through strong leadership and coordination, rapid case detection and isolation, aggressive contact tracing, and strict quarantine measures,” the CDC said.
Media sites such as the BBC, the Star and publications such as the Policy Forum have also reported on Vietnam’s proven effective response to the pandemic.
Claim 2: Excessive borrowing over the last four years has placed Ghana in a high debt risk category
Verdict: Even though Ghana is in high-risk debt distress category due to excessive borrowing, it is not as a result of events of the last four years. Ghana has been in this category since 2015 when an IMF and World Bank report published in April 2015 concluded Ghana to be so on account of breaches in the debt-service to revenue ratio.
Two documents were accessed to ascertain this claim.
The first document titled Joint Ghana World Bank-IMF Debt Sustainability Analysis document dated December 2019, an analysis of Ghana’s joint bank-fund sustainability, shows that Ghana’s risk of external debt distress and overall risk of debt distress were truly both high.
“External and overall debt are at high risk of debt distress… Nonetheless, debt is assessed as sustainable thanks to favourable market access, the authorities’ commitment to macroeconomic stability and fiscal discipline, and the potential for steeper than assumed fiscal consolidation. In the short term, fiscal discipline is necessary to ensure debt sustainability and maintain market confidence, but external factors, including worsening global risk sentiment, still pose significant risks,” the IMF document reads.
However, Mahama’s assertion that this is a result of excessive borrowing specifically from over the last four years is inaccurate as we found Ghana’s categorisation by the IMF was since 2015.
An IMF Ghana report on the ‘Request For A Three-Year Arrangement Under The Extended Credit Facility’ (pg13&14) published in April 2015 also judged Ghana’s debt at a high risk distress.
“The Debt Sustainability Analysis (DSA) concludes that Ghana is at a high risk of debt distress, on account of breaches in the debt-service to revenue ratio over 2015–17 and after 2021. The authorities are committed to limit their borrowing plans to loans with a minimum grant element of 35 per cent, with possible exceptions in line with the debt limits policy… Bank of Ghana gross financing to the budget in 2015 will be limited to 5 per cent of previous year’s revenue, using only marketable financial instruments”, the report read.
In 2015, the IMF stated in the report that Ghana’s public debt continued to rise at an unsustainable pace, however, in the 2019 report, the IMF judged Ghana’s debt as sustainable.
Another document titled, The fall and rise of Ghana’s debt jointly published by the Integrated Social Development Centre Ghana, Jubilee Debt Campaign UK, SEND Ghana, VAZOBA Ghana, All-Afrikan Networking Community Link for International Development, Kilombo Ghana and Abibimman Foundation Ghana in October 2016 was accessed to verify the claim.
The document, in analysing how Ghana had at the time, ‘fallen in a new debt trap’, also shows that Ghana was categorised as a high risk of debt distress by the World Bank in 2015.
“In April 2014 Ghana was assessed as at moderate risk of debt distress but ‘approaching high-risk levels’. At the next review in March 2015 this changed to being confirmed as at “high risk of debt distress”. Yet, seven months later in October 2015, the World Bank broke its own rules based on its own assessment by giving a guarantee for (high-cost) bonds for a country rated as at high risk of debt distress,” the document reads.
Therefore, even though Ghana is in a high risk of debt distress category due to excessive borrowing, it is not a matter of the last four years as Mahama claimed. Ghana has been in this category since 2015 when an IMF and World Bank report published in April 2015 concluded Ghana to be so on account of breaches in the debt-service to revenue ratio.
Conclusion
Conclusively, from the claims identified in Mahama’s introductory speech at the NDC Manifesto launch 2020, one was true and another was false.
On Sunday, President Akufo Addo addressed the nation on measures taken to contain the spread of the COVID-19 pandemic. In his address, the President announced the re-opening of Ghana’s air borders on September 1 and outlined a number of measures. Among the measures, passengers who enter the country are required to have proof of a negative COVID-19 PCR test and are mandated to undergo COVID-19 testing upon arrival at the Kotoka International Airport.
The next day, the government convened a press briefing to provide further information about the arrangements. At that press briefing, the deputy health minister, Dr Bernard Okoe Boye, justified the $150 mandatory COVID-19 test to be done at the airport by making comparisons with what pertains in other countries (40:32 – 42:25).
“When you go to a place like Zimbabwe, you will pay about $210 for the test. In China, you will pay about $150 for the test and they are doing PCR which is a very good test that identifies the virus itself …Now when you go to Togo here, you will pay about 150 euros, not dollars. In fact, I just got the figures for Nigeria – you will pay about $130 and not only that, you need to go to a hotel and wait for results, which can be one or two nights…,” Dr Oko Boye said.
The verification of the claims was limited to the specific countries mentioned by the deputy health minister. Before anything, it is important to provide some explanation about COVID-19 testing.
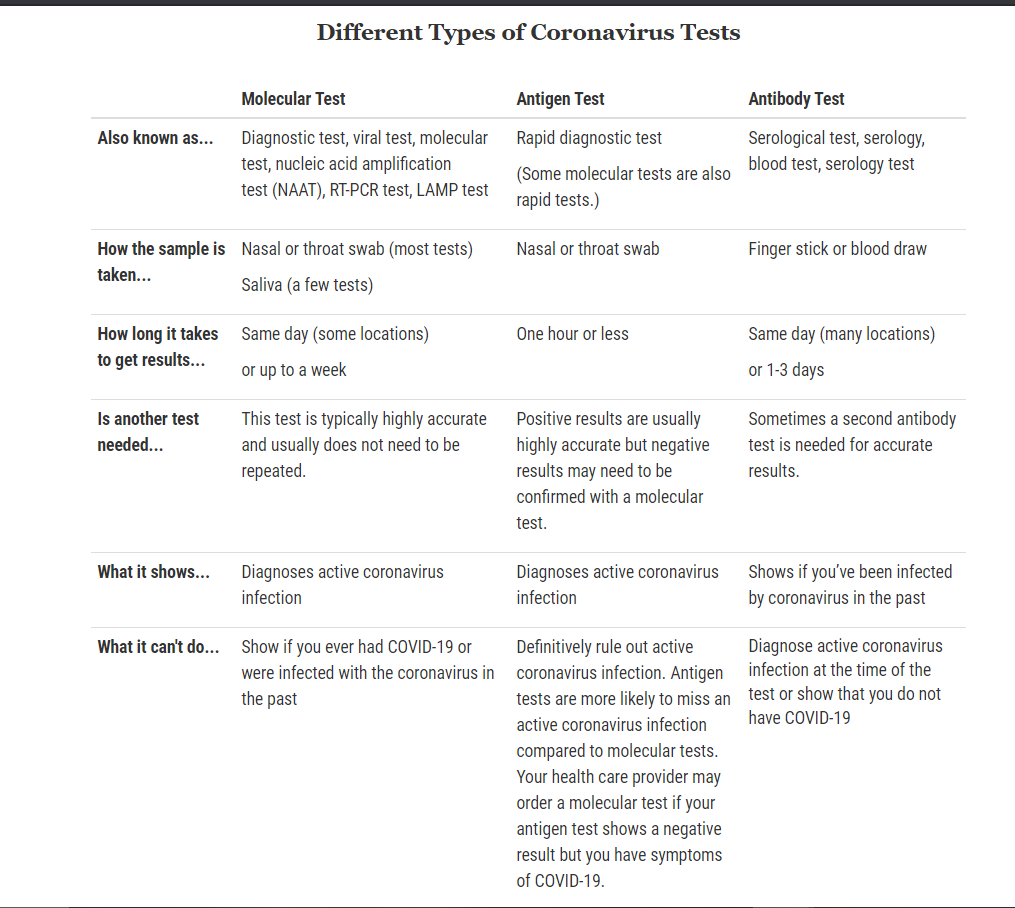
Types of COVID-19 tests around the world
Tests for COVID-19 are categorized into three types namely PCR (Polymerase Chain Reaction) test, antigen test and antibody (serology) test. PCR is a test that looks for bits of the SARS-CoV-2 which is the virus that causes the COVID-19 in the nose and other areas of the respiratory tract. It determines if a person has an active infection.
Antigen test looks for pieces of the protein that constitutes the SARS-CoV-2 virus to determine if a person has an active infection. An antibody test is a serological test that looks for antibodies against SARS-CoV-2 in the blood to determine if there has been a past infection.
Although both PCR and Antigen tests determine if there’s an active infection of the COVID-19, PCR is more expensive and takes more time than the antigen test.
A number of countries, Iceland, France, Germany, and Russia, including are conducting COVID-19 testing at airports.
Ghana’s testing regime
Travellers arriving into Ghana since the resumption of passenger flights on September 1 are required to present proof of a negative COVID-19 PCR test taken not more than 72 hours before the scheduled departure from countries.
On arrival, all passengers are to undergo mandatory COVID-19 testing. This test according to Dr Okoe Boye should not last more than 30 minutes and will come at a cost of $150 to be borne by the passenger. The type of testing being done at the Kotoka International Airport is the antigen test.
Government officials say the amount of $150 was reached upon a careful analysis of what happens elsewhere in other countries. In defending the price, the Dr Okoe Boye mentioned Zimbabwe, China, Togo, Benin and Nigeria.
We sought to verify the costs for tests in these countries as mentioned by the Deputy Health Minister.
Claim 1: “Now when you go to Togo here, you will pay about 150 euros, not dollars.“
Verdict: False
Togo confirmed its first case of the COVID-19 on March 6 2020. As of September 2, 2020, the Africa Center for Disease Control reported that the country had 1416 total confirmed cases, 28 deaths and 1035 recoveries.
The government of Togo announced the closure of all borders on Friday, March 20, 2020. All non-essential inbound and outbound traffic and travel was prohibited per that order with only cargo allowed into the country.
International and domestic flights resumed in Togo on August 1, 2020, with the announcement of COVID-19 protocols.
First, all travellers both departing and arriving are mandated to register and fill an online traveller declaration form on the government’s website. Any traveller departing from Lomé must undergo a COVID-19 PCR test within 72 hours before departure.
A laboratory dedicated to screening passengers departing from Lomé is set up in the enclosure of the old terminal of Gnassingbé Eyadema International Airport (AIGE) for COVID-19 screening tests. Again, any passenger entering Lome has to present a negative PCR test dating less than 5 days before boarding.
Upon arrival, the passenger is subjected to another PCR test. For this purpose, they must complete the online form available and pay the cost of the said test before their departure. The on-site PCR test that passengers undergo at the airport upon arrival is CFA 40,000 which is equivalent to $72 US and approximately £55.
All travellers must install TOGO SAFE, a contact tracing application, upon arrival at the Lomé Airport. It is mandatory for the app to remain activated for at least 30 days. Passengers who do not install the app are quarantined in a containment facility provided by the government for at least 14 days.
The cost of the quarantine is borne by the traveller. Test results arrive within 24 hours. Those with positive test results will be required to self-isolate either at home or at a government facility until they test negative.
From the foregoing facts, we find the claim made by the Deputy Health Minister that passengers pay 150 euros for the test false. The cost of the on-site PCR test done at Lomé Airport is less than €100.
Claim 2: When you go to a place like Zimbabwe, you will pay about $210 for the test.
Verdict:False
Zimbabwe reported its first case of the novel coronavirus on 21st March 2020. It now has a cumulative case count of 6559 cases, deaths stand at 203 while 243 persons have recovered from the COVID-19.
On Monday, March 24, 2020, Zimbabwe’s President, Emerson Mnangagwa, announced the closure of the country’s borders to all human traffic except for returning residents and cargo. He announced then that returning residents will be subjected to strict screening procedures including a 21 day self-quarantine.
At the moment, Zimbabwe is closed for passenger flights. Only Zimbabwean nationals are allowed into the country.
Zimbabwe’s Information Minister Monica Mutsvangwa says “the plan is to start with the resumption of domestic flights and then move to international flights” adding that “Government is finalizing on modalities for the reopening of airports to support the resumption of the tourism sector.”
Since Zimbabwe’s air borders are still not opened for international flights, protocols only relate to returning citizens.
We checked with Zimbabwe’s Health Ministry about COVID-19 arrangements for returning citizens. An official from the Epidemiology and Disease Control(EDC) department told Starr Fm’s correspondent in Zimbabwe that citizens who arrive are to be tested. The official, however, added that government facilities do not have the capacity to test at the moment so travellers are referred to private centres to do the test. The cost of the test is therefore dependent on the institution where the test is done.
The Health Ministry says it is not aware that travellers are charged $210 to take the COVID-19 test at these private centres although in the past some persons have taken the test at a cost of $65.
The EDC official says travellers can either be quarantined at government institutions or private institutions. We did an online search about private institutions offering COVID-19 packages, below is the one from the Bronte, The Garden Hotel, Harare, Zimbabwe.
We therefore rate this claim false.
Claim 3: ‘For Nigeria, you will pay about $130 for the PCR test and not only that, you need to go to a hotel and wait for results, which can be one or two nights…’
Verdict: True
During a media briefing at the Nnamdi Azikiwe Airport in Abuja, Chairman of the Presidential Task Force(PTF), Boss Mustapha, announced that Nigeria’s borders will open to air passengers on September 5.
As stated at the briefing, all travellers to Nigeria must have tested negative within 96 hours of departure.
“All intending travellers to Nigeria must have tested NEGATIVE for COVID-19 by PCR in the country of departure pre-boarding. The PCR test MUST be within 96 hours before departure and preferably within 72 hours pre-boarding. For certain countries, COVID-19 PCR tests will only be acceptable from specified laboratories.”
Travellers must again repeat the PCR test upon arrival in Nigeria on the 7th day of arrival in Nigeria.
According to the National Center for Disease Control ( NCDC) in Nigeria, a traveller, upon arrival in Nigeria is to undertake a COVID-19 test for which the individual will pay independently.
Dubawa was told by NCDC officials that an amount of ₦50,000 is to be paid to have the PCR test conducted upon arrival in either Lagos or Abuja airport. This is equivalent to about $129.30.
Some private laboratories however charge between ₦40,000 to ₦50,000.
Claim 4:In Benin, you pay €150 for the PCR test.
Verdict:True.
A COVID-19 testing centre has been set up at the main airport in Cotonou, Benin’s capital. All travellers to Benin are to be subjected to a mandatory PCR test upon arrival at a designated government site. The cost of the test is in two forms, normal service and premium service.
With the normal service, passengers are to pay 100,000 FCFA (an equivalent of about $165) which covers the test on departure and on arrival and 14 days after arrival in Benin. This is equivalent to €152.45.
For the premium service, passengers pay 125,000 FCFA (equivalent to €190.56) for their test on departure from and return to Cotonou. For this service, passengers are guaranteed ease and speed in sample collection, a 6-hour turnaround time for the results, and service at a VIP center. Travellers, upon having their samples taken, may be directed to self-quarantine while waiting for their results.
Should a passenger be found positive of COVID-19, all other tests that are carried out are free of charge and may be subject to government-mandated isolation measures. However, if the individual requires premium service, an additional 25,000 FCFA is charged.
All these charges are at the passenger’s expense.
Claim 1: In China, you will pay about $150 for the PCR test.
Verdict: False.
According to our sources at Taiwan Fact-checking Center, the cost for PCR test in China is CHY 120 which is equivalent to $18. Travellers arriving in the country are to take the test and then proceed on a 14-day quarantine in specific hotels. The hotels cost about CNY 350, equivalent to $51 daily but vary depending on the city and hotel. Meals are also available at the travellers’ expense. Travellers have the option of taking a second test in the last few days of quarantine.
Further, information from the Chinese Ministry of Foreign Affairs, the Civil Aviation Administration of China and the General Administration of Customs indicate that passengers are required to provide evidence of a negative test result before boarding a flight to China.
“In order to ensure the health and safety of international travel and reduce the risk of cross-border transmission of the epidemic, passengers on flights coming to China will be boarded with a negative certificate of the new coronavirus nucleic acid test,’ a joint statement reads.
‘Chinese and foreign passengers who come to China by flight shall complete the nucleic acid test within 5 days before boarding. Testing should be carried out in institutions designated or recognized by Chinese embassies and consulates abroad.
Passengers of foreign nationality shall apply to the Chinese Embassy or Consulate for a declaration of health status with a negative nucleic acid test certificate,” it added.
This then implies that prices may vary depending on the health centre the individual may test at. It is, therefore, unlikely to have the same price across all test centres or health institutions.
The cost of the COVID-19 nucleic acid test (NAT), similar to what is being called the PCR test, was in April relatively cheaper than in other countries. In April, a test cost between $22 to $37 in China but was about $500 to $3,000 in many other countries.
The reason for this disparity, according to a study, includes the fact that
China has adequate production capacity and supply of test reagents.
The Chinese government adopted a policy of blending government-guided prices with market-regulated prices which keeps the pricing low and standardized.
Logistics companies and third-party testing institutes provided great support, reducing other added costs of the testing reagents. For instance, some companies provided free transportation services to ensure the smooth flow of medical supplies.
Dubawa has reached out to Chinese authorities for an official statement regarding test charges for travellers and will update this report once information is made available.
………………
This fact-check was originally published by StarrFmfactchecker but has been edited and updated by Dubawa
The information ecology has in the recent past been inundated with materials that have often proven to be either misleading or completely false after subjecting such information to thorough scrutiny.
The preponderance of such information has not only become widespread but has also largely polluted the information ecosystem, putting the end receivers of information at risk of taking actions that may be injurious to their person or the greater society.
These misrepresented facts, commonly termed ‘fake news’ (Shu et al, 2018), manifest in forms such as satire, false context, imposter content, manipulated content, false connection, leaks and hate speech on both traditional and social media platforms (Wardle & Derakhshan, 2017).
A more generic terminology called information disorder, as proposed by Wardle & Derakhshan, is now widely accepted in deconstructing and unpacking the large swath of contortion in the information ecosystem. The concept categorizes and contextualizes misrepresented facts into three broader scopes – dis-information, misinformation, and mal-information
The taxonomy explains dis-information as false information that is knowingly shared with an intent to harm and misinformation as false information shared without the intent to harm. Mal-information, on the other hand, refers to the use of true information with the intent to harm.
At the core of information disorder is the treatment of messages, news, and facts in media spaces; and the expanse of information disorder typology has further enabled the deconstruction of media messages for researchers to better understand the import of disseminated information. Often, treatment of the media messages is explained within the context of media framing.
Nonetheless, how media messages are presented or framed for audience consumption and the angle or perspective from which a news story is told is not always the exact representation of reality but rather a reconstruction from various angles of a small section of reality.
Framing of messages and images in the media in the wake of the outbreak of the coronavirus has reignited the debate on how the media treat and represent reality. Thus, in the coverage of the COVID -19 pandemic, the media, more often than not, presents reality from the perspective from which they observe events and unfolding actions in society (Critical Media Review, 2015).
Therefore, the dichotomy between information disorder and framing of media messages is widely amplified in the coverage of the COVID–19 pandemic (UNDP, 2020). In most cases, the treatment of stories on the pandemic is characterized by an avalanche of misleading information presented on media platforms and the frames into which these media messages are presented accentuate the thematic underpinnings that constitute information disorder.
An evaluation of selected media messages is analyzed in this text to highlight how media framing of the pandemic is laden with paradigms spawned by constructs of information disorder. A postmodern perspective in assessing information is applied in evaluating the various media frames and situating them within the broader spectrum of information disorder.
Media Framing of the Pandemic
Since the World Health Organization (WHO) declared the coronavirus diseases a pandemic, media organizations and media platforms have been giving attention to all aspects of the pandemic. Key among them are media assertions of a found cure or a supposed cure for the disease that is causing a global meltdown and killing tens of thousands of individuals across continents.
In Ghana, for example, the first two cases of infection from the virus were reported on March 12, 2020. Since then, the cases have spiralled and have crossed the 40,000 marks, causing over 200 deaths. The state of confusion that the virus has thrown the world into has made all persons edgy and are readily clutching onto any information without verification, so long as it will help save them from the ravaging impact of the virus. In telling their story, the media has given varied slants to the perspectives from which it reports on the COVID-19 pandemic. It ranges from stigmatization, fear peddling, false hope to pseudo-science.
Stigmatization
The novel coronavirus disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first detected in December 2019 in Wuhan, a city in China’s Hubei Province with a population of 11 million, after an outbreak of pneumonia without an obvious cause. The virus has now spread to over 200 countries and territories across the globe, and was characterized as a pandemic by the World Health Organization on March 11, 2020 ( Zhu, Wei, & Niu, 2020).
Headlines across the media spectrum have been buzzing with stories on the pandemic. However, the visibility given to the pandemic is sometimes diluted with information that is quite worrying. Media headlines such as one attributed to the President of the United States of America calling the virus the ‘Chinese Virus’ and another newspaper headline ‘coronavirus made in china’ were but a few of the reports that did not only stoke the flames of stigmatization against the Chinese but also portrayed china as the cause of the world’s woes.
Though it is factually correct to trace the origin of the pandemic to homeland China, a further association and renaming of the pandemic as a Chinese virus or a virus made in China is a subtle stigmatization of the People’s Republic of China as carriers of the virus. In Ghana and some other parts of the world, some medical equipment from China were either received reluctantly or rejected outrightly, in fear that since they are coming from China, they may have been compromised. This phenomenon, also amplified by newspapers on their front pages is a typical example of mal-information within the information disorder spectrum – though it is true that the origin of the virus can be traced to China, media slants to the publications soiled the image of the country in the eyes of the world at large.
Fear peddling
Media reportage on the pandemic again suggested strongly that the aged are most at risk when they contract the virus to the extent that death appears inevitable. This representation in the media on one hand emboldens the youth to disregard safety protocols and on the other hand creates fear in persons in the 65 and above age bracket.
The overarching effect of such media representations has reinforced a sense of security for one generation and a no hope situation for the other in the face of the ravaging effect of the pandemic. Though evidence from many countries has suggested that the aged fell quickly to the virus, it was not exclusively a risk prone situation only to the oldies. Some media reports showed that children and the youth were also vulnerable to the virus, thus eventually causing their deaths. In Ghana, some medical practitioners in their prime have lost their lives while battling the disease.
Media portrayals of the aged as risk-prone to the diseases while the youth are risk-averse to the pandemic are thus misleading. A better story may have been told if the picture painted in the eyes of the public had been that the virus does not discriminate between ages and that all persons are at risk of the virus’ capacity to infect and destroy people, regardless of age.
False Hope
Traditional and social media platforms have been flooded with a multiplicity of information to the effect that extracts from hibiscus flower (sobolo), a concoction made from the neem tree and a certain Madagascar tonic are considered by many as the surest antidote to the cure of COVID -19. Some media reports suggested further that countries in the tropics who are exposed to the harsh humid conditions from the sun are less likely to contract the disease.
The framing of such stories to suggest an African cure to the pandemic flies in the face of WHO’s continued insistence that there is still no known cure for the virus; hence, the suggestion that some plant extracts can cure the disease is not only false but is also willfully propagated to mislead.
Pseudo-science
Media reports on the COVID-19 pandemic are not devoid of pseudo-science. Technology has been widely attributed to the cause of the pandemic. Particularly mentioned is the emergence of 5G technology. Media reportage of 5G technology as the source of the coronavirus pandemic caused public uproar in some countries.
As often as experts continue to debunk a linkage of the pandemic to the technology, the media through its coverage gave credence to it. While originators of the information know the falsity of the information and still go-ahead to distribute such, others unknowingly redistribute a ‘false information’ they have believed in.
Implications
The increasing rate of information disorder comes with its implications. Generally, end receivers of information may take one action or the other based on a piece of information that its credibility is wobbly. Indeed, the acceptance by a section of the public that 5G may be the cause of the pandemic resorted to the destruction of 5G equipment in some developed countries. The act of destruction is borne out of fear that the technology, when fully implemented, will threaten the existence of the human race.
Also, the belief that some herbs hold the magic wand for the cure of the corona virus resulted in a number of persons trying any medication or herb that is reported in the media to fight the virus. The Madagascan tonic was touted as the invention that is here to save the world; ironically, its healing prowess is not full proof and the country continues to record increasing coronavirus cases with some deaths long after popularizing its own remedy for the virus.
As media messages fail to meet the expectations of the audiences, they will be dismissive of media messages. The phenomenon may result in audiences ignoring very important information that will need their support towards the promotion of the well-being of society.
Conclusion
It is evident from the discussion that the media is as powerful as it is in informing on key policies and serving as a conduit in promoting behavioural change, but misleading information on media platforms can create unnecessary anxiety and create a schemata for judging people. Framing of media messages often accounts for the contorted reality that the public is exposed to. The media, thus have a role in consciously ensuring that news and all other news enhancements are not skewed to mislead the audience across the globe.
Again, as cases of information disorder in all its forms – misinformation, disinformation, and mal-information – soar, fact-checking every claim has become a vital arsenal in media literacy, a weapon that will enable consumers of media messages to subject media publications to thorough scrutiny to ascertain the factual basis of the information distributed.
Bibliography
Critical Media Review (2015, October 19). What is framing? Retrieved from What is Media Framing?
Shu, K, Sliva, A, Wang, S, Tang, J, & Liu, H. (2018). Fake News Detection on Social Media: A
The researcher produced this analysis under the auspices of the Dubawa 2020 Fellowship to facilitate the ethos of “truth” in journalism, to enhance media literacy in the countryand to contribute to a body of knowledge on information disorder in the country.
With the dying interest in stories regarding coronavirus in Ghana at a time that the country’s preparations for elections are getting into high gear, not much is in the news about the pandemic ravaging the world. As periodic information about the global disaster remains important for most aspects of public and private life, here is an update.
According to the World Health Organisation (WHO), the global confirmed case count for the Covid-19 pandemic currently rests at 18,902,735 as at August 7 with a death toll of 709,511 across 216 countries, areas and territories.
Updates from Worldometer, on the other hand, reports that the global death toll for the COVID-19 pandemic is now at 721,857 as at August 7, 2020, with 19,477,842 confirmed cases presently.
Although the data varies slightly, it is clear that there is an increase in cases across the world. All is not lost however as 12,025,753 recoveries have also been recorded worldwide.
In Ghana specifically, infections continue to rise as confirmed counts reach 40,097 as of August 7, 2020, according to reports on the Ghana Health Service (GHS) website.
Recoveries and discharges are also at 36,638 and 206 deaths. It is important to note that recoveries and discharges do not correlate even though reported as if they do. This is to say that an individual may be discharged without necessarily having recovered from the virus. This is because of the new discharge policy in effect since June 2020.
As stated by the President in his latest and 14th address to the nation on Covid-19, more and more restrictions have been eased in the country in the bid to restore some normalcy. All these changes are to take place with continued adherence to safety protocols.
Here are some of the changes:
Increase in church service duration from one to two hours and the restriction on the number of congregants worshipping at a time has been lifted as of August 1, 2020. This is to say that there is no limit to the number of congregants to be present in worship centres henceforth. However, the safety protocols, social distancing, mask-wearing, and handwashing and sanitizer usage remain. Well-ventilated service spaces are prescribed for worship periods.
Opening of tourist destinations and open air drinking spots sites excluding nightclubs, pubs and the like.
Full capacity in transport vehicles like taxis, buses etc
COVID-19 is still an ongoing threat to every individual, regardless of age, colour, social status, or nationality, thus making the need for constant update essential, even as the country prepares for general elections.
The Director-General of the Ghana Health Service, Dr Patrick Kuma-Aboagye, says COVID-19 does not spread fast in buses.
Studies have proven that contracting COVID-19 on publictransport is far less likely than it was earlier feared.
Full Text
In phase two of the easing of restrictions, President Akufo-Addo, in his 14th Address to the Nation on updates to Ghana’s Enhanced Response to the Coronavirus Pandemic on Sunday July 26th, lifted the restrictions in the transport sector.
“In consultation with the Ministries of Transport and Aviation, and the leadership of transport operators, Government has taken the decision to lift the restrictions in the transport sector and allow for full capacity in our domestic airplanes, taxis, ‘trotros’ and buses,” the President said.
Following that announcement, Dr Patrick Kuma-Aboagye, Director-General of the Ghana Health Service (GHS), came out to explain that COVID-19 does not spread fast in public transports.
“Our advice to allow all forms of transportation services to resume full operation is that, based on our contract tracing activities, we have had cases all over but we have not found anyone who traced the infection through transport,” Dr Kuma-Aboagye said.
He backed his claim further by saying the evidence so far in the country did not support the risk of transfer of COVID-19 in vehicles compared to other diseases.
Verification
Some scientists had earlier predicted that crowded public transport could stifle Africa’s fight against COVID-19. The likelihood of the transmission of the virus in public transports resulting from overcrowding led health experts to recommend mitigating protocols like social distancing or spacing in vehicles.
This concern for managing the challenge of COVID spread in a confined setting within which people congregate led the Africa Centres for Disease Control and Prevention to develop some guidance for the transportation sector.
This, however, triggered its own complications, as in South Africa, where it was reported that social distancing was affecting the country’s dysfunctional and vital public transport with commuters struggling to get transportation to destinations and drivers recording losses.
Dubawa conducted internet research and found some contact tracing studies and research conducted elsewhere which found fewer cases of COVID-19 infections in public transportation.
A recent study conducted by researchers at Sante Publique France, the National Public Health Agency and published on June 4, 2020, identified 150 COVID-19 infections and found that none of the 150 cases was traced to any form of transportation.
A similar study in Austria found that not one of 355 case clusters in April and May was traceable to those in transit.
Also, a cluster of COVID-19 disease in communities in Japan between January and April, 2020 came to a conclusion that fewer percentage of “super-spreader” events was traced to public transport.
However, the studies revealed that the likelihood of contracting COVID-19 was higher in offices, restaurants and bars.
The daily mail reported on its website on August 3 that there was no available data in the UK about the risk of contracting COVID-19 on public transport.
The report added that analysis of contact tracing data by Sam Schwartz, a former New York City traffic commissioner, found that only four per cent of 1,300 of COVID-19 hospital admissions in early May had used public transport prior to infection.
We further spoke to Dr Kwabena Sarpong, Deputy Director of GHS in Charge of Public Health in the Central Region, to get an understanding of the transmission of the virus in public transport. He said that people are at low risk of contracting COVID-19 in public transport.
“I know some works have been done which suggests that there is a low risk of contracting the virus in public transport compared to other places but that does not also mean it is impossible to contract it in public transport,” he said.
He further explained that people are not likely to talk, sing, and shout in buses and indicated that the virus spread through droplets from an infected person through speaking, singing, coughing, and sneezing.
“If you are in a public transport loaded to capacity, you have to exercise personal responsibility and ensure that you wear the approved face masks and also make sure you or the person sitting close to you does not talk or shout,” he added.
Conclusion
Contracting COVID-19 on public transport is far less likely than it was earlier feared. Although it is not 100 per cent certain that one can not contract COVID-19 in public transports, its infection rates, according to studies, are very low.
The reporter produced this fact-check under the auspices of the Dubawa 2020 Fellowship in partnership with Ghana News Agency to facilitate the ethos of “truth” in journalism and to enhance media literacy in the country.